|
The following document lists key information about both prolotherapy and perineural injection treatment (PIT). The latter term was introduced by John Lyftogt of New Zealand. There is more information under the pages "Comparing Prolo and PIT" and "Prolotherapy Q & A" and it is useful to review each.
|
Prolotherapy: This is injection with the goal to repair weakened or stretched ligaments or tendons or stabilize joint surfaces affected by arthritis. The term prolo in prolotherapy refers to the effect of injection to grow (proliferate) new cells that form ligament or tendon tissue (fibroblasts) or stabilize or repair cartilage (chondrocytes). Prolotherapy (called regenerative injection therapy by many) can be performed using dextrose, platelet rich plasma or stem cells. Platelet rich plasma is stronger in stimulation of repair than dextrose and stems cells are stronger than platelet rich plasma, however, dextrose prolotherapy is the most commonly performed method for a number of reasons:
1. It is safe, comparable to the safety of acupuncture, as long as physicians have been fully training in needle placement methods.
2. It uses very low cost and readily available sterile dextrose solutions.
3. Prolotherapu using dextrose is the only method of prolotherapy that can be used to treat complex cases that require treatment of many areas simultaneously for benefit.
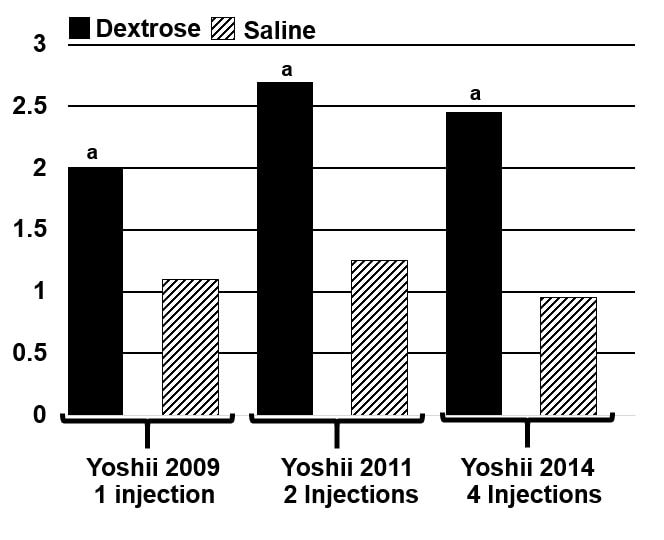
4. Dextrose has proven ability to grow normal ligament tissue. Studies in the Mayo Clinic Orthopedic Research Laboratory showed doubling of ligament thickness with dextrose injection compared to saline injection. Below are the results of 3 separate studies, showing the same outcome, (doubling of dextrose thickness side) and the new tissue took more force to rupture and was completely normal tissue on biopsy. It is also useful to be aware that this used only 10% dextrose which does not cause inflammation (12.5% or higher dextrose does). So dextrose, by itself, without inflammation can stimulate repair. If you want to link to the latest article in the series, click on Yoshii 2014 study.
1. It is safe, comparable to the safety of acupuncture, as long as physicians have been fully training in needle placement methods.
2. It uses very low cost and readily available sterile dextrose solutions.
3. Prolotherapu using dextrose is the only method of prolotherapy that can be used to treat complex cases that require treatment of many areas simultaneously for benefit.
4. Dextrose has proven ability to grow normal ligament tissue. Studies in the Mayo Clinic Orthopedic Research Laboratory showed doubling of ligament thickness with dextrose injection compared to saline injection. Below are the results of 3 separate studies, showing the same outcome, (doubling of dextrose thickness side) and the new tissue took more force to rupture and was completely normal tissue on biopsy. It is also useful to be aware that this used only 10% dextrose which does not cause inflammation (12.5% or higher dextrose does). So dextrose, by itself, without inflammation can stimulate repair. If you want to link to the latest article in the series, click on Yoshii 2014 study.
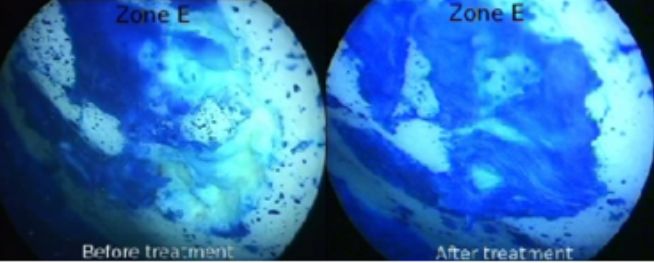
5. Dextrose has been shown to stimulate some cartilage cell growth. Note, this does not resurface joints but the goal is to stabilize and calm the joint surface in arthritis. See the picture below from our study publication (primary author Gaston Topol) showing (on the right) new growth of cartilage after dextrose injection, filling in a hole in the surface of bone. Note, this does not resurface joints but the goal is to stabilize and calm the joint surface in arthritis.
6. Research on dextrose prolotherapy is the least affected by drug company or device company bias because there are no profit motives to publish positive results. Research is typically done by physicians sacrificing their time and personal finances. Despite that challenge, high quality trials have been published in many areas and are in process in others (see research tab). Despite modest sample sizes, numerous rigorous randomized controlled trials have reported a clinically meaningful effect of dextrose prolotherapy in 11 areas (knee osteoarthritis, temporomandibular dysfunction, rotator cuff tendinopathy, lateral epicondylosis, wrist pain, finger/thumb osteoarthritis, sacroiliac pain, hip osteoarthritis due to hip dysplasia, Osgood-Schlatter disease, Achilles tendinosis, and plantar fasciosis.) Reeves KD, Lam SKH, Rabago D. Chapter 9: Therapeutic dextrose injection: Prolotherapy, perineural injection therapy and hydrodissection. In: Williams CJ, Sussman WI, Pitts JA, eds. Atlas of interventional orthopedics proceduresm, E-book: Elsevier 2021.
7. Other than the information offered by clinical trials, which is considerable, a general estimate is often made that 80% of patients should respond that have failed other treatments. That is a reasonable statement, but with three qualifications. First, complete elimination of pain and complete functional restoration are to be strived for and that depends on complete diagnosis and complete treatment. Second, the use of perineural injection treatment (PIT) has substantially affected the success rate in combination with prolotherapy, and its application is spreading worldwide as well. Third, pain is from nerve inflammation and there are multiple environmental contributions to nerve inflammation and these may need to be identified in the most difficult cases. A general observation by this author is that the percentage of responders continues to improve as expertise with combination treatment grows worldwide, and with more complete identification of environmental factors.
7. Other than the information offered by clinical trials, which is considerable, a general estimate is often made that 80% of patients should respond that have failed other treatments. That is a reasonable statement, but with three qualifications. First, complete elimination of pain and complete functional restoration are to be strived for and that depends on complete diagnosis and complete treatment. Second, the use of perineural injection treatment (PIT) has substantially affected the success rate in combination with prolotherapy, and its application is spreading worldwide as well. Third, pain is from nerve inflammation and there are multiple environmental contributions to nerve inflammation and these may need to be identified in the most difficult cases. A general observation by this author is that the percentage of responders continues to improve as expertise with combination treatment grows worldwide, and with more complete identification of environmental factors.
PIT: This is injection with a goal to restore normal function in nerves that cause chronic pain and degeneration. Approximately 40% of our sensory nerves are protein producing and designed to stimulate either 1) comfort and health or 2) pain and degeneration in structures that they supply. Nerve inflammation occurs when these nerves are producing pain-and-degeneration-producing proteins. Nerve inflammation is not reversed by arthritis medication (ibuprofen, naproxyn, or prednisone/steroid), which instead work on inflammation from the traditional (arachidonic acid pathway) inflammation. Nerve inflammation is much more common than arachidonic acid pathway inflammation, but both types of inflammation may be present. This explains why patients given steroid injections often will temporarily improve, but pain returns because nerve inflammation is ignored. Here are some high points about treatment of nerve inflammation. (See research tab for details that support statements made below)
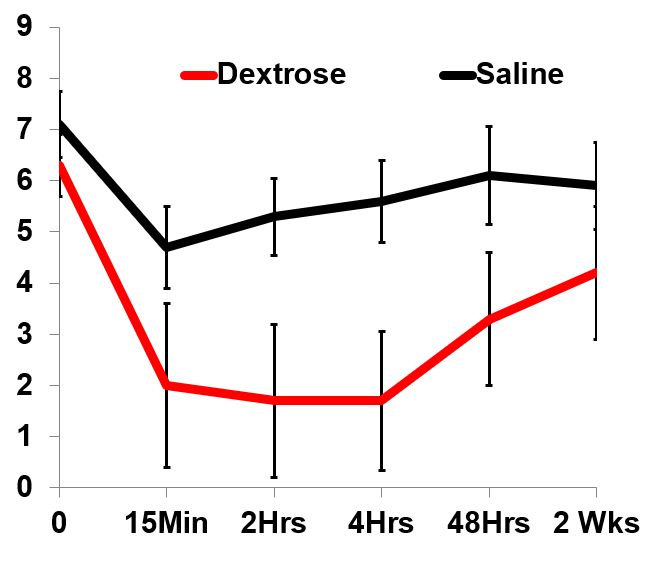
1. Dextrose treats nerve inflammation. High quality research has shown a prompt analgesic effect of dextrose injection. The speed of this response indicates that the effect of the pain producing proteins has been neutralized but the mechanism of this is complex. The graph below shows the reduction in pain after injecting dextrose versus saline in the caudal epidural space. (A place tht steroids are often injected) Within 15 minutes the dextrose reduced pain much more than saline.
1. Dextrose treats nerve inflammation. High quality research has shown a prompt analgesic effect of dextrose injection. The speed of this response indicates that the effect of the pain producing proteins has been neutralized but the mechanism of this is complex. The graph below shows the reduction in pain after injecting dextrose versus saline in the caudal epidural space. (A place tht steroids are often injected) Within 15 minutes the dextrose reduced pain much more than saline.
2. Nerve inflammation may be accompanied by local warmth or swelling. Blood vessels under the skin may dilate, causing warmth, and blood vessels become "leaky" causing local swelling.
3. Nerves have to move as you move, and when nerves are inflamed, they swell, making it easier for them to become caught or compressed. This swelling may be seen on ultrasound for some of the larger sensory nerves. Nerves move through the body in fascia, thin layers of white tissue that can encase them a bit too tightly. Because they often have a long path to travel to go around bones, through muscles, etc., they can be compressed at multiple locations.
4. Treatment may be superficial (just under the skin), treating the nerves as they dive down from skin level which is often one point of compression, or it may be deeper, locating where these nerves are compressed and injecting dextrose in those locations to pull them loose from the compressing tissue (hydrodissecting them, or in other words pulling them loose (dissecting them) without a scalpel, with fluid (hydro) effect alone. When dextrose fluid is used to jet the nerve free from the tissue in which it is encased, ultrasound shows the nerve pulling loose and, in the process, changing from a flattened to a round shape.
5. Sensory nerves that are inflamed are classically able to produce a great variety of sensations such as itching, burning pain, sharp pain, aching pain, numbness, and tingling.
6. Because these are sensory nerves, as they become affected, they do not carry sensation correctly and numbness, that typically comes and goes at first, is noticed. This is the type of compression that causes the numb hand during the night when sleeping on a shoulder or holding the arm up when driving.
7. Nerves that are inflamed do not like to be still for long periods, often causing limitations of sitting or standing or sleeping for long periods, and they also do not like to be moved back and forth a lot. Thus, either overuse or no use may increase symptoms. 8. When these nerves are malfunctioning a lot, a doctor may diagnose "small fiber neuropathy". This is a good description because these are small nerves, as compared to motor nerves and some big sensory nerves that have other purposes. Opathy means disease of, so neuropathy means disease (or dysfunction of nerve). Although nerves that are inflamed long enough may have portions of the nerve malfunction permanently, showing abnormal findings on a biopsy of the nerve. Those that treat nerve inflammation are finding that most of the time these nerves are merely turned off, and can be turned on with relief of pressure and restoration of function. Even when there is an underlying process that damages nerves, such as diabetes, treating compression can be very helpful.
3. Nerves have to move as you move, and when nerves are inflamed, they swell, making it easier for them to become caught or compressed. This swelling may be seen on ultrasound for some of the larger sensory nerves. Nerves move through the body in fascia, thin layers of white tissue that can encase them a bit too tightly. Because they often have a long path to travel to go around bones, through muscles, etc., they can be compressed at multiple locations.
4. Treatment may be superficial (just under the skin), treating the nerves as they dive down from skin level which is often one point of compression, or it may be deeper, locating where these nerves are compressed and injecting dextrose in those locations to pull them loose from the compressing tissue (hydrodissecting them, or in other words pulling them loose (dissecting them) without a scalpel, with fluid (hydro) effect alone. When dextrose fluid is used to jet the nerve free from the tissue in which it is encased, ultrasound shows the nerve pulling loose and, in the process, changing from a flattened to a round shape.
5. Sensory nerves that are inflamed are classically able to produce a great variety of sensations such as itching, burning pain, sharp pain, aching pain, numbness, and tingling.
6. Because these are sensory nerves, as they become affected, they do not carry sensation correctly and numbness, that typically comes and goes at first, is noticed. This is the type of compression that causes the numb hand during the night when sleeping on a shoulder or holding the arm up when driving.
7. Nerves that are inflamed do not like to be still for long periods, often causing limitations of sitting or standing or sleeping for long periods, and they also do not like to be moved back and forth a lot. Thus, either overuse or no use may increase symptoms. 8. When these nerves are malfunctioning a lot, a doctor may diagnose "small fiber neuropathy". This is a good description because these are small nerves, as compared to motor nerves and some big sensory nerves that have other purposes. Opathy means disease of, so neuropathy means disease (or dysfunction of nerve). Although nerves that are inflamed long enough may have portions of the nerve malfunction permanently, showing abnormal findings on a biopsy of the nerve. Those that treat nerve inflammation are finding that most of the time these nerves are merely turned off, and can be turned on with relief of pressure and restoration of function. Even when there is an underlying process that damages nerves, such as diabetes, treating compression can be very helpful.